Essential Minerals for Health and Well-Being
Eight minerals run roughly eighty percent of the systems that send people to specialists, and the standard blood panel tests for almost none of them. The named mechanisms, the exact doses, and the protocol that restores the set.
The fatigue that sends you to a doctor, the 3 a.m. wake-up, the fog that will not lift, the immune system that catches everything, almost all of it traces to eight minerals your standard blood panel never measures. They run roughly eighty percent of the systems involved. Restoring them is cheap, the subjective markers move inside weeks, and mainstream medicine ignores it because there is no patent on a rock.
Your doctor measures iron and B12. Here are the eight they do not. The food on your plate was bred for yield, not for the elements every cell needs to do its work, and the one mineral the food industry pushes hardest, calcium, is the one you most over-load with, and the one whose harm in excess is least understoodfootnoteMayer, A. M. B. (1997). British Food Journal. "Historical changes in the mineral content of fruits and vegetables." Comparison of 1936 UK govt food tables vs 1991 tables found reductions of 19% in Mg, 27% in Ca, 49% in iron, 24% in K across 27 vegetables. The 2004 USDA follow-up by Davis et al. confirmed the direction across the US food supply..
Calcium is the brake. Magnesium is the accelerator. Get the relationship between those two wrong and the body slowly turns its own structure against itself.
The modern body is rarely sick from what is in it. It is sick from what is missing.
What you get back
Each item below has been mapped in the literature. None of it is folklore.
- Sleep depth. Muscle cramping, eye twitches, the 3 a.m. wake-up, all classic magnesium-deficiency signals, resolve in days once cellular magnesium starts to load.
- Morning clarity. The cognitive fog that selenium-and-iodine deficiency produces lifts as the thyroid's active-hormone conversion comes back online.
- Cardiac signal. A coronary calcium score that stabilises or regresses over years instead of climbing. The single best predictor of cardiac events we have, brought under nutritional control.
- Bone density without dairy. Calcium routed by K2 and boron into the matrix where it belongs, not deposited indiscriminately in arteries and joints.
- Immune resilience. Zinc, selenium, and vitamin D at sufficiency mean a working antiviral response and a working heavy-metal handler.
- Mood and anxiety floor. Magnesium gates the brain's excitatory chemistry; restoring it drops the baseline noise the nervous system has to fight.
- The compounding one. A body running on the minerals it was built to run on, instead of struggling against the absence of them.
What gets returned is the working version of a body most adults have never met.
The mineral that runs everything
Magnesium runs the body's energy system. It sits at the centre of every leaf of chlorophyll, the same job iron does inside the red blood cell, which is why eating greens delivers it directly. Inside the cell, magnesium stabilises the molecule you burn as fuel (), runs the pump that keeps calcium out of places it does not belong, balances the brain's two main on/off signals (), builds the body's master antioxidant, and turns vitamin D into its active form. Run short on magnesium and every one of those systems slows at once.
It is also, by a wide margin, the most under-supplied mineral in the industrial diet. puts more than half of Americans below the daily intake their own conservative benchmarks call adequate. A standard blood test misses it, because the body defends magnesium in the blood by pulling it from cells and bones. The only test worth running is , the one that reads it inside cells, and most adults sit in the lowest third of normal or below.
Then the consequences cascade. Low magnesium means the cellular fuel runs poorly, which means the pump that holds calcium out of cells runs slowly. Calcium accumulates inside the cell where it should not be (in health there is ten thousand times more calcium outside the cell than inside), and the cell's own power plants gradually . The energy system slows further. Dr. H. Ray Evers calls it the vicious cycle: not enough magnesium to make energy, not enough energy to run the pump calcium needs, the power plants calcifying as a result.
"It's like going through life with the emergency brakes on. Calcium is the brake. Magnesium is the accelerator.", Dr. Evers
Where calcium goes wrong
If magnesium is the accelerator, the next question is what happens when the brake is on without it. About 99% of the body's calcium is in teeth and bone. The remaining 1%, circulating in blood and dispersed across soft tissue, is where the harm happens when magnesium is insufficient.
A fifth of the volume of arterial plaque is calcium. The , a simple CT scan that totals the calcium in the heart's arteries, is the single best predictor of cardiac events we have, better than cholesterol, better than triglycerides, better than blood pressure. UCLA's Dr. Matt Budoff, the most prominent champion of routine calcium scanning, puts it plainly: the total amount of coronary calcium predicts heart-disease events beyond every standard risk factor. , the slow stiffening of the heart's outflow valve, shows up in roughly 29% of people over 65, and in 2-9% of those over 75 in its severe form. Kidney stones, joint mineralisation, dental tartar, arterial plaque, pineal calcification, glandular calcification: same biochemistry, different sites.
The countries with the highest cardiac death rates correlate with the highest calcium-to-magnesium ratios in their soil and water. Australia tops the list. Japan, where daily magnesium intake reaches 560 mg, sits among the lowest. Bantu women, on 200-300 mg of calcium per day, have the lowest rate of in the world; Western women on the 1,000+ mg the dairy lobby has promoted for fifty years have the highest. The mineral sold as the answer to osteoporosis tracks, in the epidemiology, with worse bone outcomes.
There is a darker thread. The 1998 Harvard School of Public Health study of 47,781 men found that those consuming 1,500-1,999 mg of calcium daily had roughly double the risk of metastatic prostate cancer compared with men at 500 mg or less. At 2,000 mg or more, the risk rose to more than four times. The 2001 Harvard follow-up of 20,885 men found the highest-dairy quartile had 32% more prostate cancer than the lowest. The American Cancer Society's senior epidemiologist Dr. Carmen Rodriguez framed the literature accurately: there is reasonable evidence that calcium plays a role in prostate cancer development.
Magnesium controls the fate of calcium. Without it, the mineral the body needs for bone deposits everywhere it shouldn't.
None of this is an argument against calcium. The body needs it. The argument is against loading calcium without the partner nutrients, magnesium, vitamin K2, boron, that decide where the calcium ends up. Take calcium alone and you raise the level in your blood. Take it with its partners and you route it to bone where it belongs.
What blocks repletion: the modern diet
If the routing problem is solvable, the next question is why the routing went wrong in the first place. The list is consistent across the literature. The minerals industrial food has stripped, in roughly descending order of severity:
- Magnesium, soil depletion, refined grains (white flour removes ~80% of grain magnesium), low intake of leafy greens and seeds
- Iodine, replaced in commercial bread by bromide in the 1980s; iodised salt covers the bare minimum and most adults under-consume it
- Zinc, bound up in the gut by compounds in unprocessed grains, low in vegetarian diets, dropping in farm soil
- Selenium, entirely dependent on what is in the soil; large parts of the US, China, and Europe are selenium-poor
- Boron, the most under-discussed of the trace minerals. Modern diets deliver maybe 1 mg/day against an evidence-supported range of 3-10 mg
- Vitamin D3, sunscreen, indoor work, latitude, and dark skin combine to leave most industrial-world adults functionally deficient
- Vitamin K2, found in pasture-raised animal fats, fermented foods, and organ meats. Industrial agriculture and the low-fat diet stripped it out
- Sulfur, comes from sulfur-containing amino acids in quality protein; industrial protein production is sulfur-poor
- Copper, paired with zinc; deficient in both directions depending on the population
This list is the protocol below, inverted. Restore these and most of the calcification, fatigue, sleep, immune, and cognitive markers begin to correct.
The protocol
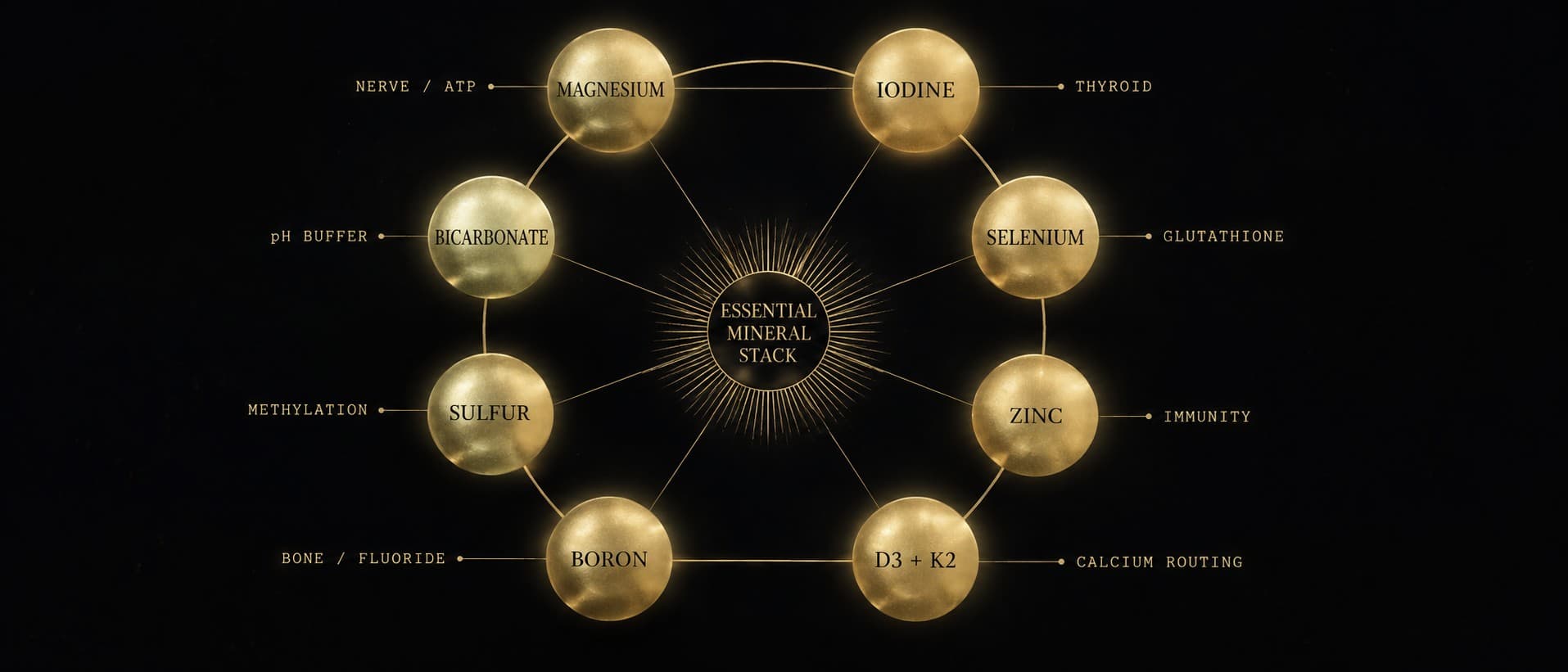
The daily stack is built around three principles: magnesium first (every other piece assumes magnesium is in place), the calcium-routing partners (D3 + K2 + boron, so calcium goes to bone and not arteries), and the iodine and detox supports (iodine + selenium + sulfur, which work on the heavy-metal and toxin load the body carries).
This is not medical advice. Doses are the doses the literature supports; the discipline is testing before, during, and after.
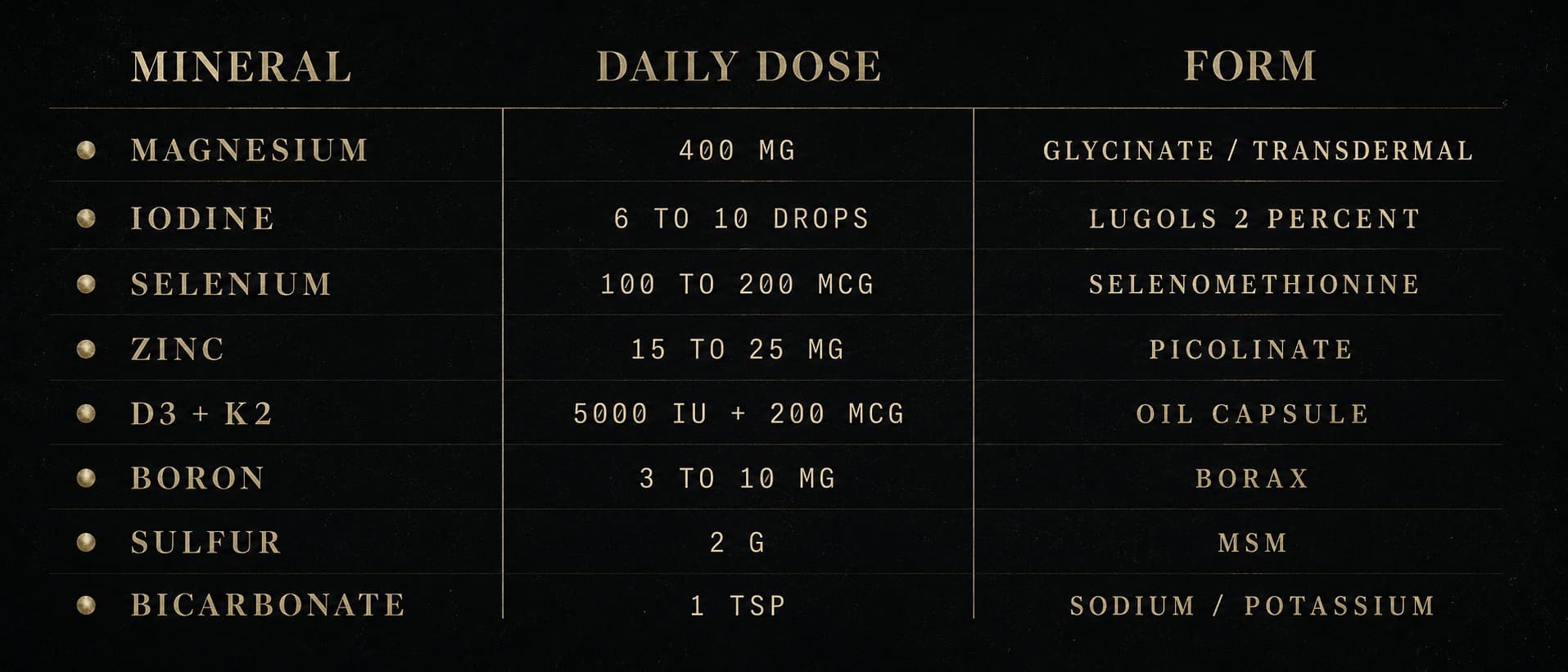
1. Magnesium, transdermal and bicarbonate, daily
The most efficient way to load magnesium is two routes in combination.
Through the skin: magnesium chloride hexahydrate, Zechstein or Ancient Minerals brand. Sprayed daily on the inside of the forearms, the chest, the abdomen, and the calves after a shower. Let it sit 20-30 minutes, rinse off the residue. bypasses the problem oral magnesium has, which is that it triggers loose stools long before the body has loaded any meaningful amount.
By mouth: magnesium bicarbonate water, Mg(HCO₃)₂. The bicarbonate form is one of the best-absorbed oral magnesiums, and uniquely it delivers the alkaline bicarbonate ion alongside the mineral. For repletion without the bicarbonate angle, magnesium glycinate is the other strong oral form, the one the pineal protocol leans on; ionic and chelated forms are ranked in full in the supplement essay. The combination of magnesium chloride through the skin and sodium/magnesium bicarbonate by mouth at slightly separated times is, per Mark Sircus, the ideal way to deliver both magnesium ions and bicarbonate ions to body cells.
Target: RBC magnesium in the upper third of the reference range. Test before, test during, test after. Numbers are the discipline.
2. Iodine, Lugol's 2%, six to ten drops daily
Iodine is the master . When sufficient, it occupies the receptor sites in the thyroid, breast, prostate, ovary, and pineal that would otherwise accept fluoride, bromide, and chlorine. The high-dose iodine protocol, pioneered in the modern era by Drs. Abraham, Brownstein, and Flechas, delivers 12-25 mg of elemental iodine daily, against an RDA of 150 mcg set to prevent overt goitre.
Six to ten drops of 2% delivers approximately 15-25 mg elemental iodine. The Japanese coastal diet, which provides 12-25 mg/day from kelp, is the natural-population anchor for this dose; the public-health outcomes in those populations on hormone-sensitive cancers and thyroid disease are strikingly favourable.
Iodine loads more efficiently when selenium is adequate (selenium protects against the burst of oxidative stress as displaced halides leave). Always pair.
3. Selenium, 100-200 mcg, daily
Selenium is the partner mineral for two enzyme families that decide whether the body's detox machinery runs at full capacity: , which recycles the master antioxidant, and the that turn storage thyroid hormone into the active form.
Selenium deficiency produces a quiet hypothyroidism, low energy, cold intolerance, slow thinking, that does not show up on the standard TSH lab. Selenium also directly, forming inert compounds the kidneys can excrete. Two Brazil nuts deliver about 100 mcg if the trees grew in selenium-rich soil; selenomethionine capsules are the reliable supplement.
4. Zinc, 15-25 mg, daily
Zinc is the partner mineral for over 300 enzymes, including . It is required to convert serotonin into melatonin, which makes it rate-limiting for the pineal output discussed in the decalcification piece. It also stabilises vitamin D receptors and competes with aluminium and iron for absorption sites in the gut.
Form matters. Zinc picolinate, citrate, or bisglycinate are well absorbed. Zinc oxide is largely passed through. Take it with food.
Sustained high-dose zinc (above 40 mg long-term) can deplete copper; the rough rule is 1 mg of copper for every 15 mg of zinc. Test if running a high-zinc protocol.
5. Vitamin D3 with K2, 5,000-10,000 IU D3 + 200 mcg MK-7
This is the calcium-routing pair.
Vitamin D3 alone, without K2, accelerates the very problem we're trying to solve.
D3 increases how much calcium the gut absorbs; without K2 to send that calcium where it belongs, it deposits indiscriminately in arteries, kidneys, joints, and glands.
K2 is the cofactor for two proteins that decide calcium's fate. , the protein that routes calcium into bone, needs K2 to switch on. , which keeps calcium out of arteries and soft tissue, also needs K2 to switch on. The stays in the body for about three days, so one dose covers the day. Take it with the evening meal alongside some fat for absorption.
Test 25-OH vitamin D in serum, target the upper end of the reference range, around 60-80 ng/mL.
6. Boron, 3 to 10 mg, daily
Boron is the trace mineral the modern diet has most quietly lost. It supports cell membrane integrity, regulates inflammation, amplifies the action of vitamin D and magnesium, and of bone and soft tissuefootnoteThe boron content of food has declined with industrial agriculture; supplementation at 3-10 mg/day shows benefits across multiple endpoints from bone density to cognitive performance in the Pizzorno 2015 review.. It is also, and almost no one says this out loud, one of the most direct dietary levers on testosterone the body has.
Boron raises free testosterone, the bioavailable fraction that does the work rather than the portion bound up and inert, while it lowers oestradiol and the inflammatory markers and nudges vitamin D and DHT upward. In a controlled trial, ten milligrams of boron a day, the amount in a small dose of borax, raised free testosterone by more than a quarter and dropped oestradiol inside a single weekfootnoteNaghii, M. R. et al. (2011). Journal of Trace Elements in Medicine and Biology. One week of 10 mg/day boron raised free testosterone by roughly 28 percent, lowered oestradiol, raised DHT and the free-to-total testosterone ratio, and cut the inflammatory markers hsCRP and TNF-alpha.. Walter Last's survey of the literature reports the same lever at a higher setting: around a hundred milligrams of borax a day raised free testosterone by a third in younger men, which is precisely why it has quietly become a bodybuilder's mineralfootnoteLast, W. (2012). "The Borax Conspiracy." Available at yummy.doctor. A survey of boron's history and physiology, its role in bone, joints, the parathyroid, and sex-hormone metabolism, and the regulatory campaign that reclassified a cheap mineral as a poison.. Free testosterone up, oestrogen down, inflammation down, joints and bone recovering faster, the exact profile an athlete chases, from a mineral that costs almost nothing.
The source is , and there is only one borax. It is a single naturally-occurring mineral, sodium tetraborate decahydrate, mined as a soft evaporite crystal from the beds of dried ancient lakes, chiefly in Turkey, which holds most of the world's reserves, and in the Mojave Desert of California, the deposit the twenty-mule teams hauled out of Death Valley a century ago and the name still on the box. The powder in the laundry aisle and the powder a pharmacy would sell you are the same compound from the same ground, and by weight borax is roughly as acutely toxic as table salt. The warning not to eat it is regulatory, not chemical: a cheap, unpatentable mineral that competes with arthritis and hormone drugs gets labelled a poison rather than a remedy. All borax is food-grade borax.
Dose it small, because it is powerful. An eighth of a teaspoon of borax dissolved in a litre of water and sipped through the day delivers about seven milligrams of elemental boron, inside the supported three-to-ten range and enough to move every marker above. That is the whole daily dose. You do not scale it up because it is working; boron is a potent biological signal, not a bulk nutrient, and the benefit lives at the bottom of the dose curve, not the top. Start at the smaller end, hold there, and stop if you notice any irritation.
7. Sulfur, MSM or DMSO, daily
Sulfur is the third-most-abundant mineral in the body. It is the raw material for the sulfur-containing amino acids, and through them, for glutathione, the body's master antioxidant. It is required to build collagen (the protein in skin and connective tissue), to produce bile, and to run the liver's reactions.
Two delivery routes:
- MSM (), taken as coarse organic sulfur crystals, 1-3 g/day in water. Source matters here more than almost anywhere else in the stack. Most commercial MSM is the cheap synthetic powder run off an industrial process and can carry its solvent residues and anti-caking agents; what you want is MSM distilled from natural plant lignin and sold as plain crystals with nothing added. Buy the organic crystal, not the synthetic powder.
- DMSO (), the precursor the body converts into MSM. Topical (joints, wounds) at 70% solution. Pharma-grade only; the industrial-grade DMSO is contaminated.
For day-to-day mineral support, MSM is the workhorse. DMSO is the surgical tool for specific applications.
8. The bicarbonates, sodium and potassium
A sodium-and-potassium-bicarbonate formula taken daily delivers two things: the alkaline bicarbonate ion (which the kidneys use to balance the body's daily acid load), and potassium (which most modern diets are short on against the sodium they over-deliver).
is the body's first line of defence against the daily acid load it generates from food, stress, and exercise. As acid builds up, bicarbonate gets consumed; chronic acid loading depletes the body's bicarbonate stores and pulls minerals out of bone to compensate. Supplying that buffer directly, for a few cents a day, is the whole of the lemon and bicarbonate essay.
Daily pH monitoring is cheap and direct. Urine pH should run between 6.5 and 7.5; saliva should run 7.0-7.4. Strips cost less than the supplements they measure.
The arc
Mineral repletion is not a one-month project. Magnesium loading, measured by RBC labs, takes 60 to 120 days to show meaningful change in a chronically depleted adult. Iodine sufficiency, measured by a 24-hour urine collection after a 50 mg loading dose, takes a similar window. Coronary calcium scores stabilise or regress over years, not weeks.
The subjective markers show up earlier. Sleep depth and morning clarity in 2 to 4 weeks. Muscle cramping, eye twitches, sugar craving, all classic magnesium-deficiency signals, resolve in days. Skin and hair quality (sulfur, zinc, copper) take 8 to 12 weeks. Cognitive markers (iodine, selenium, thyroid downstream) take 3 to 6 months.
The discipline is consistency. The reward is a body running on the minerals it was built to run on, instead of struggling against the absence of them.
Treat the system as a body. Treat the body as a system.
The minerals are the ground. They are what the body is built from, and what it has been quietly starved of. But the stack rests on something even more elemental, the eighth item already pointed to it: the acid-base balance that decides, hour by hour, whether your bones get to keep the minerals you just put back. That balance can be tilted with two things already in your kitchen, a lemon and a spoonful of bicarbonate, and that is where the work goes next.
Sources
- The Magnesium Miracle,
- Magnesium in man, implications for health and disease, . https://pubmed.ncbi.nlm.nih.gov/25540137/
- Calcium intake and prostate cancer (Harvard SPH 47,781-man cohort), . https://pubmed.ncbi.nlm.nih.gov/9521168/
- Vitamin K2 and the calcium paradox,
- Iodine deficiency in industrialized countries,
- Selenium in human health and disease, . https://pubmed.ncbi.nlm.nih.gov/22381456/
- Boron in human and animal nutrition,
- Comparative effects of boron supplementation on plasma steroid hormones and proinflammatory cytokines (J. Trace Elem. Med. Biol., 2011),
- The Borax Conspiracy, . https://yummy.doctor/wp-content/uploads/2021/04/Borax-conspiracy.pdf
- Vascular and Systemic Calcification (IMVA, 2024),
- Sodium thiosulfate for treatment of calcific uremic arteriolopathy,
Next in the series
The Incorruptible Body · The GroundLemon and BicarbonateThe five-cent morning drink that hands the body back its acid-base buffer, and the chemistry of why it works.
- Published
- Reading
- 13 min
- Sources
- 11