The Supplement Buyer's Manual, Why Less Is More and How to Choose What Works
Most supplement tablets are 80 percent filler and a poorly absorbed remainder. The fillers to refuse on sight, why ionic and liquid beat tablet, and the minimum effective daily stack.
Open the multivitamin in your cabinet and weigh what you are actually paying for. Fifty milligrams of active sits inside four hundred milligrams of wood pulp, and the white coating that makes it look pharmaceutical is a nanoparticle banned across the European Union since August 2022. You bought a pressed disc of industrial filler with a trace of nutrition pressed into it, in a chemical form your gut absorbs at four percent. The supplement industry is a $180 billion freight train running on one assumption, that more is better, and the consumer runs on a second, that a green leaf on the bottle means it is good for the body. Neither premise holds.
The discipline that does work is small. Choose few. Choose ionic or chelated. Choose natural over synthetic. Refuse the fillers. Most people violate every one.
A supplement the body cannot absorb is a supplement being excreted, after the body has paid the metabolic cost of trying to process the filler matrix it arrived in.
This is the buyer's manual to the essential minerals piece. That essay named the eight elements every adult needs to restore. This one is how to actually restore them without the industry capturing the budget and the body.
The principle of fewer
The first rule of supplement discipline is that the stack should be small. The second rule is that it should be smaller than that. Most people walk into a Whole Foods aisle and come out with fifteen bottles, each compelling at the shelf. The body cannot integrate fifteen things at once. The absorption of any one drops as it competes for the same transporter sites with the other fourteen. The cost is high, the compliance collapses inside a month.
The shape that works is the inverse: six to eight core items running daily, dosed to clinical levels, tested for actual response, rotated against the lab markers. The ninth and tenth are rarely additive. Usually one displaces a core item and total benefit drops.
This is the model pharmacology already runs. is now understood to produce worse outcomes than the conditions it was meant to address, and the last decade of practice has moved aggressively toward deprescribing. The same arithmetic governs your cabinet. The stack does not have to be long. It has to be right.
The fillers to refuse on sight
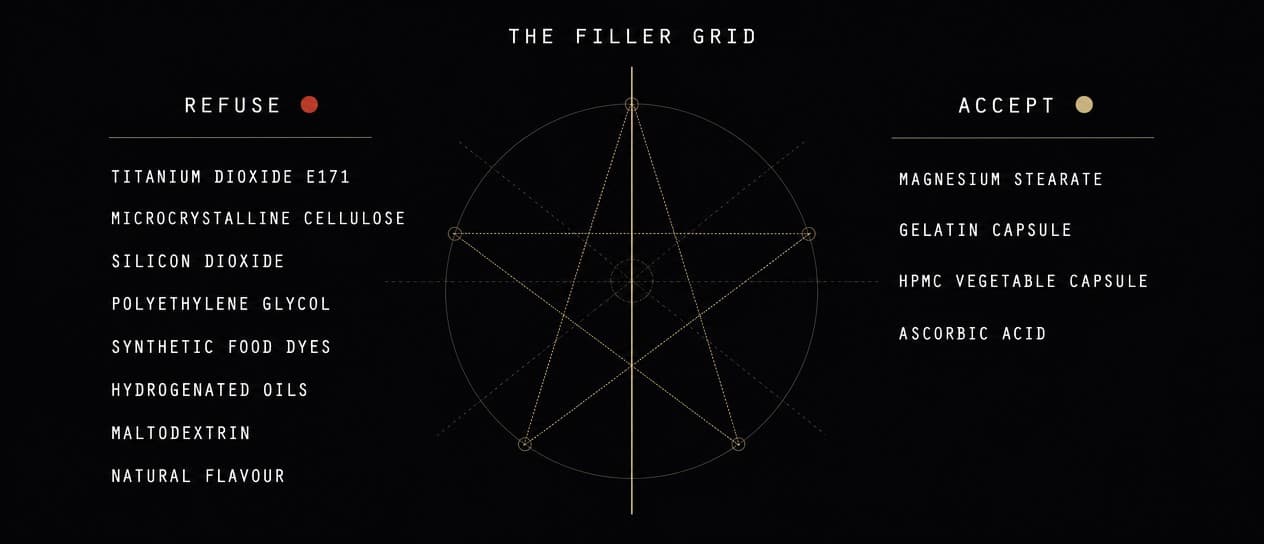
In a tablet, the active ingredient is usually a minority of the mass. The rest is the manufacturing matrix: the bulk that holds the pill together, the lubricant that lets it run through high-speed presses, the coating that makes it swallow easily and look pharmaceutical. Some of it is inert and acceptable. Several items are not. The non-negotiable refusal list.
Titanium dioxide (E171)
A whitening agent in tablet coatings and capsule shells, banned as a food additive across the European Union as of August 2022 after the that genotoxicity could not be ruled out and no acceptable daily intake could be set. The US has not followed. American manufacturers still use it freely, so the label is your only protection.
The mechanism: titanium dioxide is delivered as nanoparticles. , accumulate in liver, spleen, and brain, and there is no excretion pathway for accumulated titanium. The daily dose is small. Small daily doses across forty years are not.
Refuse it. There is no nutritional justification. The manufacturer chose it to make the pill look white. Find a brand that does not.
Microcrystalline cellulose
Purified wood pulp or cotton-derived cellulose used as a bulking agent, often 50 to 70 percent of the mass of an oral tablet. The argument for it is that cellulose is plant fibre the body excretes. The argument against it is more interesting.
It is often the largest single ingredient in a vitamin pill that holds 50 mg of active and 400 mg of cellulose, and the label rarely makes that clear. It also acts as a in the gut, lowering the concentration of active ingredient at the absorption site. And a non-trivial subset of people develop hypersensitivity to it over time.
Mostly inert at moderate dose, but there is no reason to swallow it daily for forty years when a manufacturer who skips it is on the same shelf. Capsules made of plant cellulose (vegetable capsules, the standard alternative to gelatin) are a different category and broadly fine.
Silicon dioxide (SiO2, "anti-caking agent")
Synthetic amorphous silica, used as a flow agent to stop powder clumping in high-speed bottle-filling lines. The FDA defends it as GRAS (Generally Recognised as Safe) at typical food doses. The newer concern is the same nanoparticle translocation question as titanium dioxide: modulate gut permeability through the same pathway. It is in essentially every conventional supplement, ingested across decades. Refuse the major-amount exposure. There is no nutritional reason to carry industrial silica into your gut every day for forty years.
Polyethylene glycol (PEG) and PEG derivatives
A solubiliser and coating agent, and the adjuvant component implicated in mRNA vaccine anaphylaxis, now understood to be more allergenic than assumed. has risen sharply since PEG entered the food and pharmaceutical supply at industrial scale. Refuse it where you find it.
Synthetic colours and food dyes
FD&C Yellow 5 and 6, Red 40, Blue 1 and 2. Pure cosmetic value, derived from petroleum, banned for use in children's medications across much of Europe. There is no excuse for these in a supplement.
Hydrogenated oils
Partially-hydrogenated soybean oil, palm oil, or similar, used as a tablet binder. Same metabolic profile as the industrial trans fats banned from the food supply, inflammation-driving on a slow burn. Refuse them on the principle that no one would knowingly eat them as a food ingredient.
Maltodextrin and "natural flavour"
Maltodextrin is a corn-derived sugar polymer that spikes blood glucose more aggressively than table sugar in clinical glucose-response studies, used as a bulking agent and flavour carrier. "Natural flavour" is a regulatory category covering essentially anything the manufacturer wants to declare proprietary, routinely MSG, propylene glycol, and a basket of solvent residues. Both signal a low-quality formulation.
The acceptable exceptions
Two ingredients show up on most filler-warning lists that are, on the evidence, fine. They belong here so you do not refuse a clean product on the wrong grounds.
- Magnesium stearate. The most-feared filler on the wellness internet, and a flow agent at sub-1 percent concentration, derived from stearic acid (a saturated fatty acid in animal and plant fat). The claim that it forms a "biofilm" blocking absorption is biochemically unsupported; the studies that produced it measured isolated lymphocyte response, not gut absorption. The actual literature, Tebbey and Buttke's review and subsequent industry data, has produced not a single case of adverse effect at supplement-manufacturing doses. Refusing it narrows your supply of well-formulated products and gains you nothing. Let it through.
- Gelatin capsules. Pure protein, derived from beef or pork hide, the capsule shell, digested as protein. The plant-capsule alternative (HPMC, hydroxypropyl methylcellulose) is equally fine. Gelatin is not the worse option.
- Cellulose-based vegetable capsules (HPMC). Fine, as above. Differentiate from microcrystalline cellulose as a bulking agent inside the capsule. The capsule shell itself is a small amount and a different application.
The form principle: ionic, then chelated, then everything else
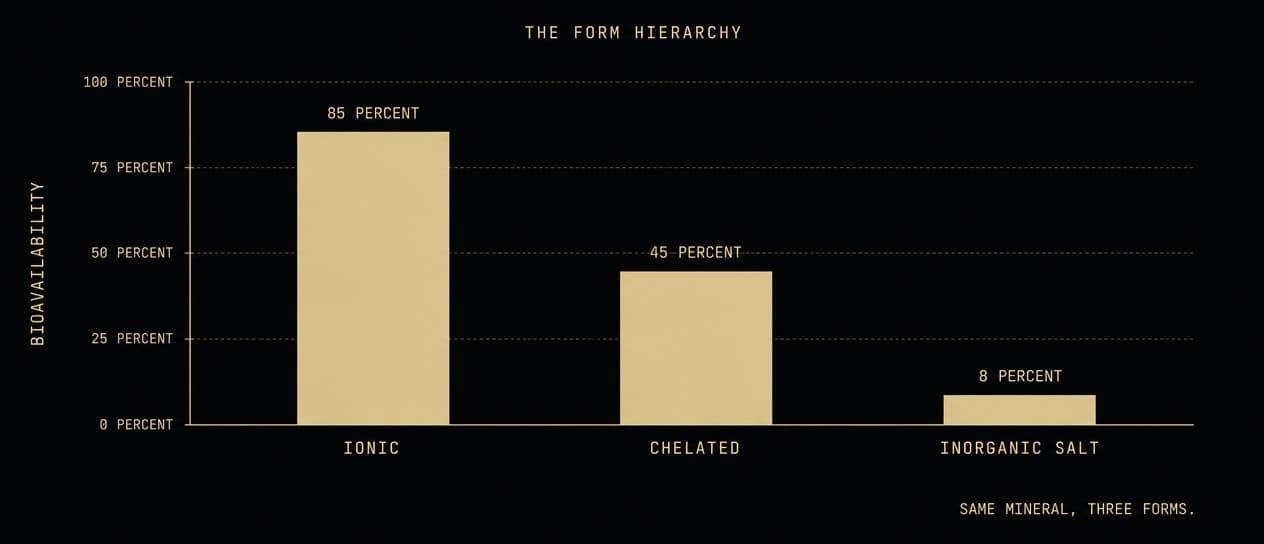
The same mineral in two chemical forms can deliver an order-of-magnitude difference in how much crosses the gut wall and reaches cells. This is the single most-overlooked variable in supplement choice, and where the consumer routinely overpays for a product the body cannot use.
Three categories, in order of bioavailability.
1. Ionic (the gold standard)
Ionic minerals are already separated into the charged atomic state the body uses. is magnesium that has already shed the carrier salt and floats in water as free Mg2+ ions. The same holds for ionic zinc (Zn2+), copper (Cu2+), selenium (selenite or selenomethionine), iodine (I- or I2), and the trace minerals.
Absorption approaches the theoretical maximum because no digestive work is needed to free the mineral from its carrier. The transporters in the gut wall pick up the ion directly. Typical bioavailability runs 70 to 95 percent, against the 4 to 30 percent of a typical tablet.
The form is almost always liquid, often a dropper delivering 50 to 250 microlitres per dose. Brands that have made the ionic case well over a long horizon: Trace Minerals Research, ConcenTrace, Quinton, Eidon. The market caught up to ionic in the past decade and the cost came down with it.
2. Chelated (a strong second)
A chelate is a mineral bound to an amino acid or organic acid the body recognises as a transport vehicle. The chelating molecule shepherds the mineral past the competition at the gut wall, gets absorbed as a complex, and releases the mineral inside the body. (most popular for magnesium and zinc), , picolinates, malates, and aspartates are the workhorse chelated forms. Citrate is the weaker case: fine for zinc and calcium, but magnesium citrate is only partly retained and stays osmotic in the gut, which is why it works better as a laxative than a repletion form.
The Albion patented glycinate technology (sold as TRAACS on many labels) is the most rigorously third-party-validated chelate on the market. The studies show absorption advantages of 2 to 4 times over the basic mineral salt and substantially better gastric tolerance.
This is the form most well-formulated tablet and capsule supplements use. For minerals where the ionic form is hard to find or unstable in liquid (iron, calcium, B-complex, the fat-soluble vitamins), the chelated form is the right default.
3. Inorganic salts (the cheap, default, and worst form)
This is the supermarket multivitamin, the chain-pharmacy "calcium," the budget "magnesium." Magnesium oxide is the worst offender: roughly 4 percent of an oxide dose is absorbed, while the other 96 percent draws water into the gut osmotically and gives the user loose stools, which the user then mistakes for a "detox effect."
The oxide, carbonate, gluconate, and sulfate forms exist in the supply chain because they are the cheapest to manufacture and carry the highest milligram-per-pill density. They have the lowest absorption. They are still listed on most generic supplements in a hospital pharmacy. Refuse them.
Why liquid beats tablet, almost always
A tablet is a pressed disc of active ingredient plus binders, lubricants, disintegrants, and often a coating. To absorb it, the body must first dissolve the binder matrix, then dissolve the active inside it, then transport it through the gut wall. Each step loses efficiency.
A liquid is already in solution. There is no disintegration step. The active is at the absorption surface the moment it leaves the stomach. , absorption begins under the tongue and bypasses the first-pass metabolism of the liver entirely.
The two specific advantages of liquid over tablet:
- No filler matrix. A 1 mL dose of a tincture is closer to 95 percent active and water than the 20 percent active and 80 percent filler of a typical tablet.
- Dose flexibility. A dropper delivers 50 to 250 microlitre increments. A tablet delivers exactly what the manufacturer fixed at the press. For minerals titrated against a lab value (iodine, zinc, copper), this matters significantly.
The cases where a tablet or capsule is the better format:
- Magnesium glycinate and other high-mass chelates. A clinical dose (200 to 400 mg of elemental magnesium) in liquid is a large daily volume; the tablet is more compact. The transdermal route covered in the minerals essay is the high-performance alternative.
- Fat-soluble vitamins (A, D, E, K). Available as liquid oil-based drops, the best format; available also as soft-gel capsules, which are fine. The dry-tablet form is the worst of the three. Take the natural forms: D3 rather than D2, natural mixed tocopherols rather than synthetic dl-alpha, and K2 as MK-7.
- Single-time-of-day, high-mass actives (creatine, taurine, glycine, MSM) are sold as bulk powder and dosed by the gram in water. That is the right format and not a tablet question at all.
Choose the methylated B vitamins
The B vitamins are sold in two grades the label treats as equal and the body does not. The cheap synthetic forms, cyanocobalamin for B12 and folic acid for folate, are not the forms the body runs on. Cyanocobalamin carries a cyanide group the liver has to cleave and discard before the vitamin is usable; folic acid has to be converted through several steps before it becomes the folate the cells actually use. Roughly four in ten people carry a common variant in the gene that throttles that conversion, so the synthetic folic acid backs up in the blood unconverted while the cells stay short, a deficiency hiding inside a full supplement.
Buy the active, methylated forms the body uses directly: methylcobalamin or hydroxocobalamin for B12, methylfolate (5-MTHF) for folate, and pyridoxal-5-phosphate (P5P) for B6. They cost a little more and skip the conversion the cheap forms gamble on. It is the same principle as ionic over oxide, applied to the vitamins: take the form the body was built to use, not the one that was cheapest to manufacture.
The case for ascorbic acid
Vitamin C earns its own line, because it runs more jobs in the body than almost any other single molecule. It is also one of the few supplements where the form barely matters: ascorbic acid is ascorbic acid, and the body uses it the same whether it came from an orange or a lab.
What it does, in short, is hold the body's tissue and its chemistry together. It is the non-negotiable cofactor for building , which is skin, blood vessels, gums, tendon, and bone; the scurvy of sailors was collagen failure for want of this one molecule. It is the body's primary water-soluble antioxidant, and it regenerates vitamin E and feeds the recycling of glutathione, the master antioxidant. It concentrates most heavily in the adrenal glands, spent under stress to build the stress hormones. It is required to turn dopamine into noradrenaline and to synthesise carnitine, and it sharply raises the absorption of plant iron.
It also pulls against the heavy-metal load of a contaminated century. Higher vitamin C tracks with markedly lower blood lead across the whole populationfootnoteSimon, J. A., Hudes, E. S. (1999). Journal of the American Medical Association. "Relationship of ascorbic acid to blood lead levels." In the NHANES III population, people in the highest third of serum ascorbic acid had a markedly lower prevalence of elevated blood lead than those in the lowest, independent of other factors., and it supports the excretion of lead, cadmium, and mercury, both by feeding the body's own chelation pathways and by neutralising the oxidative damage a loose metal does inside the cell while the body works it out. It is a cheap, daily, gentle partner to the heavy-metal work in the insulators essay.
The dose is generous, because the body holds only what it needs and excretes the rest: one to three grams a day, split across the day, more under illness or heavy detoxification.
The minimum effective stack
Combine the principles above and this is the minimum-effective daily stack for an adult on a Western diet, before any condition-specific layering.
- Liquid ionic magnesium, or transdermal magnesium chloride oil, dosed to RBC magnesium in the upper third of the reference range. The single most-deficient mineral in the modern diet.
- Liquid Lugol's iodine 2 percent, starting at 2 to 6 drops daily and titrating toward the 6 to 10 drop (roughly 15 to 25 mg) loading range run in the minerals and pineal protocols, always paired with selenium. 24-hour urinary iodine load test once a year.
- Selenium, 100 to 200 mcg/day, selenomethionine or two Brazil nuts from a selenium-rich source.
- Zinc bisglycinate or picolinate, 15 to 25 mg/day, paired with copper bisglycinate 1 to 2 mg/day if running long-term high zinc.
- Vitamin D3 with K2 (MK-7), 5,000 to 10,000 IU D3 with 200 mcg MK-7. Oil-based liquid drops or soft-gel capsule.
- Boron, 3 to 10 mg/day, as borax dissolved in water or as a boron glycinate.
- Methylcobalamin B12 sublingual, 1,000 to 5,000 mcg/day if vegetarian or vegan; 500 to 1,000 mcg/day as insurance even for omnivores over 50, when stomach acid drops and absorption falls.
- EPA/DHA, 1 to 3 g/day, from a clean wild fish oil or algal oil source.
Eight items. Every one addresses a deficiency the food supply alone, in 2026, does not reliably cover. The ninth, the tenth, the twentieth are almost always net-negative. The body cannot integrate the load, the absorption competes, the budget escalates, the compliance collapses.
Layers on top of this, for specific situations:
- For active calcification or arterial work: add IV sodium thiosulfate (physician-administered) and consider Cavadex per the minerals essay.
- For mood, sleep, or methylation work: add methyl-folate plus B12, dose-adjusted to homocysteine.
- For oxidative stress or detox work: add NAC 600 mg/day plus glutathione (liposomal sublingual or IV).
- For a vegetarian or vegan protocol: add creatine 3 to 5 g, taurine 1 to 3 g, carnitine 500 to 1500 mg, retinol from cod liver oil or a pre-formed vitamin A drop, per the companion essay on soil death and animal foods.
- For hormone substrates: add zinc, magnesium, boron (already in the core stack), plus tongkat ali or shilajit if running an androgen protocol.
The principle holds. Each layer answers a specific lab finding or a specific protocol. None is added speculatively, none is kept after the lab moves into range.
Numbers are the discipline. A supplement that does not change a lab marker in 90 days is a supplement that is not working, regardless of what it costs or how good the brand story is.
What to do with the bottle you already have
Most readers arrive here with a cabinet already bought, some good, some bad. The triage:
- Read every label. Hunt for titanium dioxide, hydrogenated oil, FD&C colours. Refuse on sight.
- Look at the form of the active. Magnesium oxide? Out. Calcium carbonate without K2? Out. Multivitamin in a tablet with eight binders and the active doses below 25 percent of daily value? Out.
- Check the source and the form. Favour the natural or methylated form over the cheap synthetic, and the maker who publishes a certificate of analysis. A synthetic active in a bottle with no published testing is the one to retire first.
- Test the lab markers. If a supplement has sat in the cabinet for six months and the relevant lab has not moved, it is not working for you. Drop it.
- Consolidate. Aim for the minimum effective list plus your specific add-ons. The 20-bottle cabinet becomes a 6-bottle cabinet inside a month.
Without the numbers, the protocol is a story.
The arc
Done correctly, supplementation is a tax adjustment for living in a century where the soil is depleted, the food is contaminated, and the daily detox burden is heavier than any prior generation's. Done incorrectly, it is the wellness industry charging you for the appearance of intervention while the body absorbs almost none of what was paid for.
The correct version is small, ionic when possible, chelated when not, natural over synthetic, liquid when the format exists, dosed against actual lab markers, disciplined enough to drop what the labs say is dead weight. Six to eight items, run consistently, will outperform a cabinet of twenty by a wide margin.
This closes the work of THE GROUND, the restoring of what the modern diet leaves out. With the minerals back in and the right ones absorbing, the body has the raw material it was starving for. The next task is the opposite motion. Now the clearing begins, with the most fundamental input of all, the one the cell burns every second and most people deliver in shallow, oxygen-starved breaths.
Sources
- Reassessment of titanium dioxide (E 171) as a food additive (EFSA Panel), . https://www.efsa.europa.eu/en/efsajournal/pub/6585
- Magnesium stearate, a literature review of safety in supplement manufacture,
- Bioavailability of magnesium oxide versus magnesium glycinate in healthy adults, . https://pubmed.ncbi.nlm.nih.gov/14596323/
- Comparative absorption of zinc picolinate, citrate, and gluconate,
- Ionic minerals, electrolyte balance and cellular hydration,
- Microcrystalline cellulose, allergic potential and immunogenicity (review),
- Silicon dioxide nanoparticles in dietary supplements (review), . https://pubmed.ncbi.nlm.nih.gov/27464589/
- Polyethylene glycol allergy, anaphylaxis and adjuvant cross-reactivity,
- Relationship of ascorbic acid to blood lead levels (JAMA, 1999),
Next in the series
The Incorruptible Body · The ClearingThe Oxygen CureYou are not one body but a colony of thirty trillion cells, and nearly all modern disease is a failure of their working conditions. The first condition is oxygen, the one Otto Warburg traced to the root of cancer.
- Published
- Reading
- 13 min
- Sources
- 9